Originally published on May 13, 2026. This is a developing situation and details may change.
By now, you may have heard news reports and social media discussions about Hantavirus, a virus circulating among guests on a cruise ship called the MV Hondius that has led to serious illness and fatalities. We’re here to break down the information you need to know right now to help you stay informed, not in fear.
What Happened With the MV Hondius Hantavirus Outbreak?
The Hantavirus outbreak originated on the MV Hondius, a cruise ship with 150 passengers, in early April.
Hantavirusis typically transmitted by rodents, but none were found on the ship. Theories emerged of a couple who had been birdwatching in Argentina and Chile and may have been exposed, without symptoms, prior to boarding.
Health officials believe the current outbreak involves the Andes strain of Hantavirus, a rare strain that has shown limited person-to-person transmission in past outbreaks.
The ship reported 11 illnesses and 3 deaths related to Hantavirus.
Where We Are Now.
Passengers have been evacuated from the ship and flown home to their countries of origin.
18 evacuated passengers now in US being monitored at biocontainment quarantine facilities in Nebraska, Kansas, & Georgia.
Passengers may be permitted to quarantine at home, under supervision.
These symptoms can take up to 42 days to appear. Families should contact their healthcare provider if they develop concerning symptoms after known exposure.
Do I Need to Worry About Getting Hantavirus?
At this time, no, unless you’ve been knowingly in direct contact with an infected person.
Unlike the start of COVID-19, public health experts are familiar with management of this virus and are closely tracking developments.
The fundamentals of good public health are critical to prevent spread of illness.
Expert sources such as the World Health Organization, CDC, and your local health department are your best place for up-to-date information.
When Should I Call My Pediatrician?
If you still have concerns, it is always a good idea to have a conversation with your pediatrician. News about emerging illnesses can feel overwhelming for parents, especially when information online changes quickly. One of the benefits of concierge pediatric care is having direct access to a trusted pediatrician who can help you understand evolving health concerns, answer questions, and guide your family with evidence-based information. We are here to partner with you and help you remain informed, not in fear!
Hot summer days with a baby can feel like a lot. Babies don’t regulate their body temperature as well as adults do, which means it’s easier for them to overheat—and harder for them to tell you when something’s off.
That doesn’t mean you’re stuck inside until things cool down—there are practical ways to help keep your baby cool and safe when temperatures rise. I talked to two experts, board-certified pediatrician Dr. Debra Goldenring, and Jen LaBracio, Babylist’s senior gear editor, who also happens to be a certified passenger safety technician (CPST), for expert tips about what to look out for and how to keep babies safe in warm weather.
🌡️ Plan Around The Heat
You don’t have to stay inside all summer—but a little planning can help outings go more smoothly. It’s a good idea to check the weather, so you know what to expect throughout the day.
Sometimes it’s less about avoiding the heat entirely and more about working around it (and adjusting expectations a little). For example, a spray bottle filled with water can double as a quick cool-down and an easy way to keep toddlers entertained. And a stroller fan also comes in handy here.
If temperatures seem like they’re going to be high, here are some tips:
Aim for outdoor time earlier or later in the day
Take shade breaks often
Bring an extra outfit in case your baby gets sweaty
👒 Dress Your Baby For the Weather
When it comes to dressing your baby in the heat, less is usually more. Babies can overheat easily, and what they’re wearing makes a big difference.
A good rule of thumb: dress your baby in one lightweight layer, like a breathable cotton bodysuit. If it feels hot to you, it probably feels even hotter to them.
What helps:
Stick to light-colored, loose-fitting clothing
You can usually skip extra layers unless you’re heading into air conditioning
Check their chest or back (not hands or feet) to gauge if they’re too warm
To check if they’re too warm, feel their chest or back—if it’s sweaty or hot, it’s time to cool things down. Dr. Goldenring adds, “In addition, their cheeks may be flushed, and they may look sweaty and may even have damp hair.”
As we begin to officially enter the Winter season, may start to feel those telltale signs of respiratory illness – a tickle in your throat, more sniffles than usual, a sharp headache. Could it be the flu? With elevated flu activity across the nation and positive cases growing in our region this month, it just might. Let’s break down everything you need to know about the flu – from symptoms and treatments, to preventative measures.
Symptoms of the Flu
Flu is the short name for Influenza, a virus that affects your respiratory system including your nose, throat, and lungs. There are 4 types of influenza – A, B, C, and D. Flu A and Flu B are what we most commonly see during our “flu season” which is typically during the Fall and Winter, with activity often peaking during the month of February.
Symptoms of flu may look similar to other illnesses, including:
Fever
Chills
Headache
Cough
Fatigue
Body aches
Sore throat
Stuffy nose
Sound familiar? A key difference in deciding if it’s a common cold or the flu is the speed of symptom onset. The common cold may start to give you hints of its arrival in the days before you feel full-blown sick, whereas the flu often gives people very sudden, severe symptoms. A popular description we also hear from patients in clinical practice is when it’s the flu, you feel like you’ve been “hit by a truck”. People infected with influenza are also at greater risk of developing secondary infections, such as ear infections or pneumonia. Consult with your healthcare provider if you are concerned about your symptoms.
How To Know If You Have the Flu
The flu is a virus and can be difficult to distinguish between other seasonal colds we get throughout the year. This is why testing is important for data, although during peak times, healthcare providers in busy environments may diagnose flu based on clinical examination and regional data vs. using a test, because laboratories may be overwhelmed and tests that are sent out may not come back in a timely manner. You may hear the term “influenza-like illness” or “ILI” which is a term used to diagnose the likelihood of flu if a specific diagnostic test wasn’t conducted. However, at Concierge Pediatrics, we will simply conduct a flu test.
A flu test is administered by swabbing deep inside the inside of the nose, called a nasopharyngeal swab. A rapid influenza diagnostic test (RIDT) is an antigen test that will determine flu presence within about 15-20 minutes. The benefit of an RIDT is that you can get results quickly while in the office or at home, but they are not as sensitive as other tests so you can test negative and still have the flu. This type of test is now more common to find over-the-counter at your local pharmacy, unlike in the past. Other tests, like reverse transcription polymerase chain reaction (RT-PCR) tests are done with a similar collection method, and then sent out to a lab for extended testing. This can sometimes only take a few hours, but depending on the time it takes to be picked up and brought to a laboratory, plus volume of total tests received by the lab, it can take up to a few days.
At Concierge Pediatrics, we run a 15-minute PCR test to guarantee quick results. We can also provide an optional respiratory viral panel test to understand what other virus your illness may be, if not influenza.
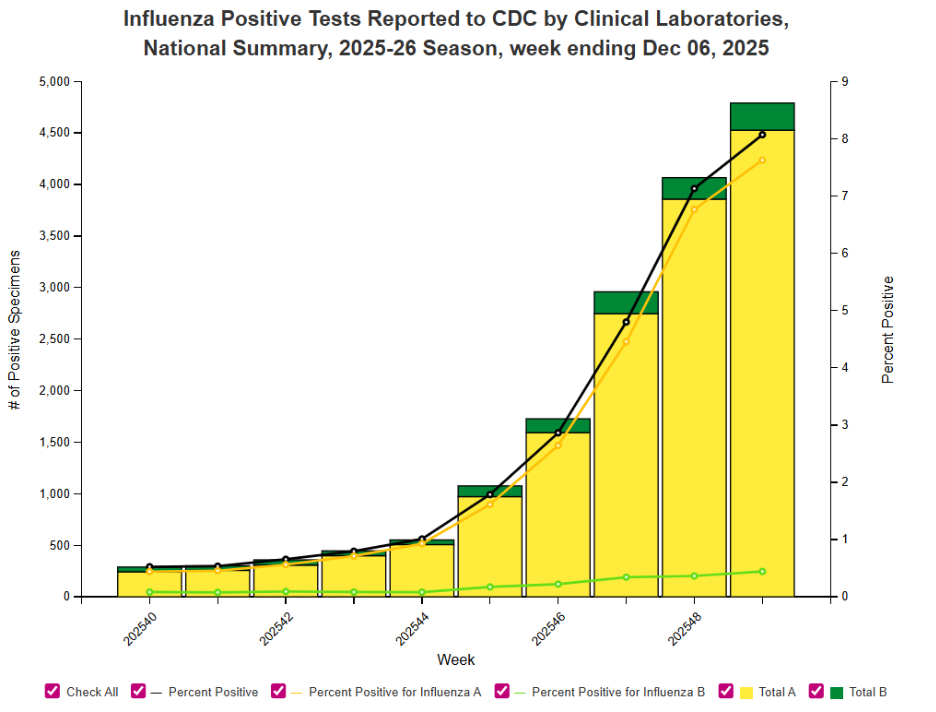
Current flu data in our region from CDC.gov
Flu Treatment and Medications
For the most part, treatment of the flu is the same as it is for the common cold. It is important to focus on the hallmarks of good self care, including quality sleep, nourishment, hydration, and rest, as well as supportive care methods to treat symptoms. Supportive care methods include a mix of medicine and proven home remedies, such as:
ibuprofen (Motrin, Advil, etc.) and acetaminophen (Tylenol etc.) for pain and discomfort from fever or body aches
honey for a cough in ages 2+ years*
cool mist humidifiers to help loosen mucous
sterile saline rinses to clear nasal passages
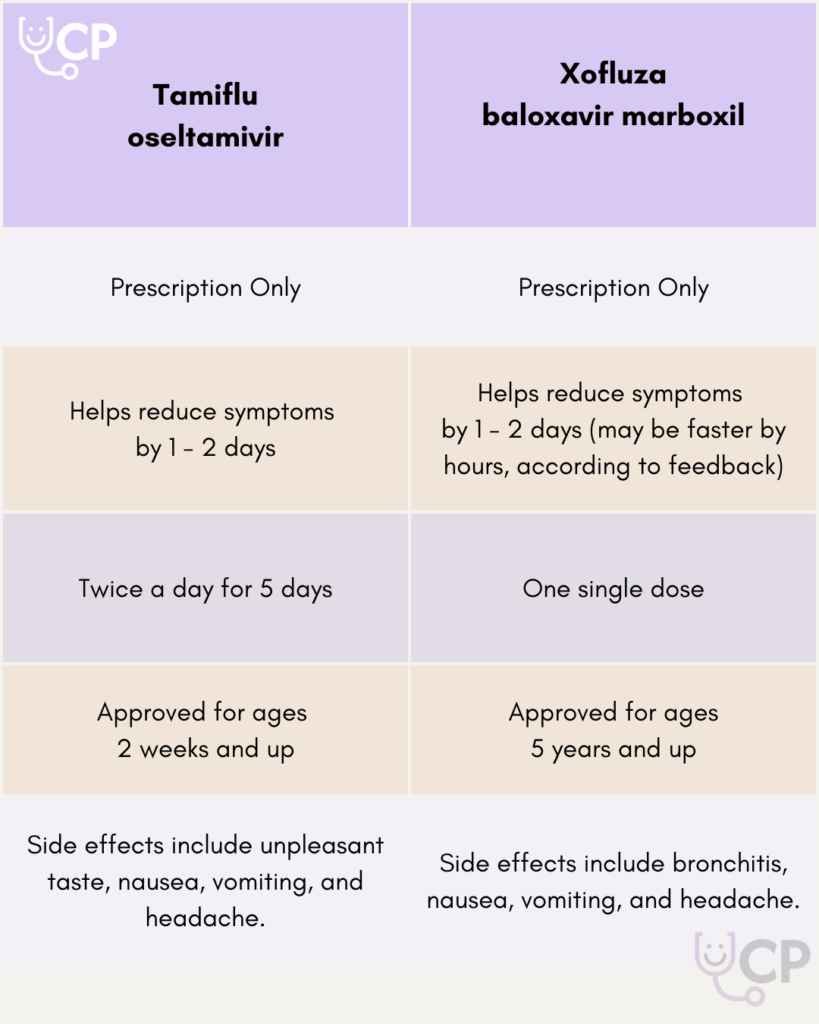
The flu is a virus, so antibiotics will not help you recover, as those are targeted to treat bacteria. However, some people may want to opt for a prescription anti-viral treatment, like oseltamivir (i.e.; Tamiflu) or baloxavir marboxil (i.e.; Xofluza). These medications are most effective when taken within 48 hours of symptom onset. Some of the drawbacks of these medications include reported unpleasant side effects, like a strong, bitter taste, nausea, vomiting, and sometimes confusion or bronchitis. For this reason, the drugs are usually recommended for immunocompromised individuals, and those under age 5 or over age 65. The benefit is that these drugs may reduce the duration of your symptoms when taken right away. Discuss the pros and cons with your healthcare provider so you can make the decision that’s best for your family!
How Can I Avoid the Flu?
The flu is an airborne illness, meaning it can spread via droplets from an infected person when they speak, cough, or sneeze. It is also possible to become infected when the droplets of an infected person touch a surface, and the next person touches the surface followed by their nose, mouth, or face.
An infected person can unknowingly spread the virus the day before they start to feel symptoms, and up to a week after becoming sick, but they are most contagious during their first 3 days of symptoms. For the sake of public health, this is why it is very important to stay home if you’re not feeling well, as much as possible, and to mask if you must leave the house when not feeling well. If a person infected with the flu is able to isolate in 1 room or area the house and use a dedicated bathroom, this will help to prevent the spread to other household members. If they’re unable to do so, they can simply follow fundamental public health measures, such as
covering their cough and sneeze into their elbow
good handwashing practices
proper disposal of used tissues
get a flu shot
Other household members should also remember to practice self care measures and frequently wash their hands with soap and water for at least 20 seconds. People with the flu can begin to return to their normal activities once they are feeling better and have been fever-free for 24 consecutive hours.
Clean high-touch surfaces, like doorknobs, light switches, countertops, bathrooms, toys, tv/gaming controls, and phones. Soap and water is usually fine, or you can use a diluted solution of household bleach and water.
Is it Too Late to Get a Flu Shot?
In the 2023-2024 season, a record 200+ pediatric deaths tragically occurred from influenza infection. The very best way to prevent the flu from hitting your household is to get an annual flu vaccine. It’s not too late to get a flu shot! Flu shots are offered at Concierge Pediatrics as part of your membership well care, and usually also for free at local pharmacies.
The flu vaccine has been researched, studied, and tested extensively for 80+ years and we do recommend getting it for ages 6 months and above. We also have the FluMist nasal spray available, so kids don’t have to feel fearful about a needle. The nasal spray is not recommended for people who are immunocompromised, nor those with asthma.
Scientists work hard to determine what the dominant flu strain is likely to be and then try to match that each year’s vaccine to the strain of flu we expect to see for the upcoming flu season. Because the flu is a virus, it means that it can evolve and still infect someone who has already gotten the vaccine. While we recognize this can be a disappointment when you feel like you’ve done the work to prevent falling ill, the important thing we will note is that the symptom severity and illness duration of a vaccinated vs. unvaccinated child with the flu are very different. If you are unsure about vaccination, talk to a trusted healthcare provider, such as any physician at Concierge Pediatrics. We will talk through your concerns and provide you with evidence-based resources to arm you with information so you can confidently make an informed decision.
The flu vaccine takes about 2 weeks to take full protection effect, and it is recommended to get the flu shot each year before Halloween (flu before Boo!), but people can be vaccinated through the month of April to be protected.
At Concierge Pediatrics, we’re here to take care of your family in health, spirit, and education. If you have flu questions, let us know! We’re here to get through flu season together.
*honey and products containing honey should NOT be given to babies under 1 year old. Honey may contain botulism spores, which are harmful to babies under 1 year old. Botulism spores are harmless for babies over 1 year old, as their immune systems and digestive tracts become more mature at that age.
Switching your baby’s formula for any reason (whether it’s not agreeing with their tummy, there’s been a recall or your brand is affected by a shortage) can be stressful, and we know it’s tough to pick the right formula for your baby in the first place. But don’t panic: “The majority of babies actually switch formulas and don’t have any difficulty,” says Dr. Victoria Regan, a pediatrician with Children’s Memorial Hermann Pediatrics.
Whatever reason for the switch, rest assured that you don’t need to worry about picking the perfect alternative—all infant formulas marketed in the US must meet the nutrient specifications listed in FDA regulations.
Below, we’ve got more specific guidance on what to look for when you need to switch, and some tips on how to make the transition go more smoothly.
If You Have to Switch Baby Formulas Quickly
If your baby’s usual formula is affected by a recall—like the recent one from ByHeart—you might need to make a switch sooner than expected. “If there is the potential for a formula contamination, going cold turkey is important to reduce any risk of illness,” says Dr. Jonathan Jassey, a pediatrician at Concierge Pediatrics based in Long Island and New Jersey. While an abrupt change can feel stressful, the good news is that most babies adjust just fine—baby formulas are all very similar due to regulations. Dr. Jassey adds, “Because the ByHeart formulas that are affected by this recall do not appear to be specialized formulas (like hypoallergenic formulas, for example), parents should be confident to just make the switch.”
If you’re switching quickly, you can introduce the new formula all at once. Some babies may experience tummy troubles (think gas or spit-up), but those symptoms usually resolve pretty quickly. If they don’t—or if you see things like blood in their stool or excessive crying—it’s a good idea to check in with your pediatrician.
Did you know that each year, approximately 12 million people in the United States are afflicted with lice? Lice have been around for thousands of years, even found on the heads of ancient mummies. A nuisance spanning generations of people with hair, these pests have a life cycle of 30 days, but left untreated, will continue to reproduce and cause a maddening itch. We connected with Russ Trichon of Lice Cops to get his take on everything you need to know about lice. Hear it from Russ himself!
About Lice
Lice are wingless insects that live on the hair of humans and feed on very small amounts of blood from our scalp. The lice cannot jump, but they can crawl from head to head, either by touching heads, sharing tools like hair brushes and combs, or possibly by laying on someone else’s pillow if a louse (singular form of lice) is crawling on it.
If I was playing Family Feud and the question was “how do we get lice” the top answer would be hugging because heads often touch during a hug! The second most common answer is selfies with other people, because heads tend to touch then, too. I especially see this from kids at school and summer camp. They may not be sharing brushes, but there sure are a lot of hugs and selfies going around! The origin story of every lice meet-cute is all about people with hair meeting other people with hair.
“Lice can affect anyone with hair. It does not discriminate by age, race, religion, or gender.“
Lice eggs, called nits, do not fall out – the only way for a nit to fall out is if you pluck the actual hair on it. This is because the eggs have a glue-like sheaththat attaches to the hair at about ¼ – ½” from the scalp. Nits have a cap called the operculum, which is like a lid on a metal trash can.
Lice can affect anyone with hair. It does not discriminate by age, race, religion, or gender. However, lice is typically more common in girls, because they traditionally have long hair, and girls hug a lot more than boys. The long hair itself is not attractive to lice, but there’s more opportunity for it to latch on to a strand when heads are touching.
The Lice Removal Process
First thing’s first – I like to calm people down during the process and talk them off the proverbial ledge, then handle the situation which luckily is a straightforward solution. A lot of people come to me very worried about their situation and I tell them this: there are things in this world that are fixable and there are things in this world that are not fixable. Lice is fixable!
A lot of people hear wrong information from family and friends and that is what brings them closer to the ledge. My job is to give them the facts and a lot of people are surprised when I don’t come with gloves or a hazmat suit because they’re thinking the worst. I like to remind them that houses do not get infested, only people get infested. More on that later.
The best way to get rid of lice is to manually remove them with a tight tooth lice comb. There are cheap versions which don’t work as well, and good versions. A good lice comb is made of strong, stainless steel with tight teeth.
At Lice Cops, I am certified in a method called the Shepherd Method, a method developed by Katie Shepherd (my hero!). This is a strand-by-strand technique that does not use chemicals nor pesticide shampoos. Lice have become more resistant to these pesticides, which is why this method is the preference of our team. Years ago, shampoos worked pretty well but we have begun to see the resistance in the form of super lice, which are increasingly unresponsive to the shampoo method. The over-the-counter products are designed to kill lice on contact, but I physically take them out. Another thing to consider is that the shampoos are not effective on nits, which use that glue-like sheath to adhere to the hair. My school of thought is that the only way to beat the bug (and their eggs) out is take them out physically.
Here’s the stainless steel, tight-tooth lice comb I like to use.
With the Shepherd Method, one treatment is usually all it takes, but I will always encourage a re-check. Although the treatments are highly effective, it is always possible for a residual nit or a baby louse to remain as part of the natural lifecycle of lice. One single louse or nit does not worry me because if they have no opportunity to reproduce, they die in about 30 days, but they may still cause an itch. Post-treatment combing, preventative sprays, and follow ups are encouraged to keep heads lice-free. It is important to remember that overcoming a case of lice is not the same as overcoming a viral illness. You cannot become immune to lice after you’ve had lice. All these things are important to think about, because you may have gotten lice from someone you’re close with, and if they don’t get checked, they may not know that they have it and can give it back to you. This highlights the importance of transparency, quick treatment, and having no shame in a lice diagnosis! The more we know, the better we can do to fight it together.
“It is important to remember that overcoming a case of lice is not the same as overcoming a viral illness. You cannot become immune to lice after you’ve had lice.“
After I give kids a treatment, I let them know that they can go back to school right away. I like to teach the parents to always follow up with the comb, use preventative sprays to reduce the possibility of reinfestation, and monitor their child for itchiness.
Lice Symptoms and How to Spot Them
Once a school sends home a notice about lice in the classroom, I am often asked by parents how to even know if a child has lice. Scalp itchiness is usually the identifying factor. If you see a little bit of redness on the nape of the neck or behind the ears, that can also be an indication of a louse bite. You can also sometimes see the lice on your child’s head. It’s better to use a good lice comb to really tell if what you’re looking at is lice.
Lice have 6 legs and adults can be seen moving with the naked eye. Babies can also be seen but are a lot smaller. Adults can be as large as the size of a sesame seed. Nits will be smaller, found within an inch from the scalp. Picture how a tiny bead of water would look on a strand of hair – that’s almost how an egg would look. It will be on one side of the strand, not wrapped around. If you run your fingers over the strand of hair and feel what is like a speedbump, it’s probably a nit. Remember that nits have a glue-like sheath that adheres them to a hair strand. If it flakes, then it’s just a dandruff flake. As I tell my clients, a flake’s gonna flake (cue Taylor Swift’s “Shake It Off”).
If you’re suspicious of possible lice, look at the scalp up to the first inch or two of hair. Because lice live off human blood, they will be found closer to their food source – the scalp. I am often asked if people should cut their long hair to reduce or prevent future lice, to which I say no. Because lice like to live in the first few inches of your hair from your scalp, cutting hair will not be effective and it will probably make you unhappy. Unless you’re excited about the prospect of a new haircut, in which case I say: do what makes you happy!
Lice Prevention Tips for Families
After someone has been treated for lice, I am often asked about lice living in the house. Since lice are topical creatures only, they will not burrow into mattresses, pillows, or cushions. I am a fan of a vacuum cleaner, which is sufficient for getting rid of possible bugs that could have fallen off hair and on to pillows, mattresses, cushions, clothes, you name it. Whatever you decide put in the washing machine will most likely be eliminated of lice, but a word of caution: as you are transferring things from the wash to the dryer, a single louse could still be alive in there, so be sure to use high heat in the dryer to be sure you’ve killed any remaining bugs. The water temperature does not matter, but the intensity of heat in the dryer will make a difference!
If you can’t put something through the dryer, be sure to separate it from everything else for a few days. A lot of people think they can “suffocate” lice and put everything in a tightened contractor bag. There’s nothing wrong about doing that, but the reality is that lice aren’t suffocated – they’re starved. Remember that lice thrive on human blood so when you have removed their food source, they starve to death in a matter of 2-3 days. You also don’t need to fumigate your home.
Lice don’t like the smell of rosemary, tea tree, or peppermint because of their strong fragrance, but many people find them quite pleasant. I am personally a fan of rosemary. There is not enough rosemary in the world to get rid of lice altogether, but because they do not like the scent, spraying in the hair prior will reduce the odds. While I think the sprays are effective, just because you have spray in your hair doesn’t mean you will never get lice. During the summertime, the sprays are less effective because kids are sweating and swimming more, which dilutes or takes the spray out. Tea tree oil and peppermint can be effective, but I personally don’t like them as much because it often gives a burning sensation to the scalp. But you’ve got choices!
If you have a friend that has lice, do not be unkind to them. Remember, lice isn’t a reflection of cleanliness or character – it’s simply a bug that anyone with hair can encounter. With the right knowledge, tools, and a little compassion, let’s remember that lice is not a crisis, it’s a problem with a solution.
About the Author
Russ Trichon is a lice removal expert and the owner of Lice Cops. Mr. Trichon was trained by head lice expert, Katie Shepherd, and has been certified through The Shepherd Institute. Lice Cops provides a kid-friendly approach, with a goal to serve, protect, and educate. Learn more about Russ Trichon and Lice Cops at licecops.com
Concierge Pediatrics is proud to share that our Founding Pediatrician, Dr. Jonathan Jassey, has been recognized by the LI Herald with the 2025 Excellence in Healthcare Award.
The Excellence in Healthcare Award honors individuals on Long Island whose dedication and commitment have made a meaningful difference in the health and well-being of others. Dr. Jassey’s lifelong mission to provide compassionate, personalized, and transformative pediatric care has not only shaped Concierge Pediatrics but has also impacted numerous families across our communities.
We congratulate Dr. Jassey on this well-deserved recognition and remain inspired by his leadership, expertise, and unwavering dedication to the children and families we serve.
Measles (also called Rubeola) is a highly contagious viral illness that spreads through the air when an infected person coughs, sneezes, or breathes nearby. The virus can linger in the air and on surfaces for up to 2 hours. It’s most recognizable by a red, blotchy rash and often begins with fever, cough, runny nose, and red, watery eyes.
How does Measles spread?
Measles spreads through microscopic respiratory droplets. It is one of the most contagious viruses, with a 90% transmission rate among unvaccinated individuals in close-contact environments.
What are the symptoms of Measles?
Symptoms usually appear 7–14 days after exposure:
High fever
Cough
Runny nose
Red, watery eyes
Tiny white spots inside the mouth (Koplik spots)
The Measles rash usually appears 3–5 days after initial symptoms, starting on the face and spreading downward. Fevers can rise above 104°F.
Is Measles dangerous?
Measles can be dangerous. While many recover without issue, 1 in 5 unvaccinated people in the U.S. who get Measles will be hospitalized. Serious complications include:
Pneumonia
Encephalitis (brain swelling)
Permanent hearing loss
Rarely, death
Infants, pregnant people, and those with weak immune systems are at higher risk.
Who is most at risk for Measles?
Unvaccinated children and adults
Infants under 12 months (too young for routine MMR vaccination)
People with weakened immune systems
Individuals in areas experiencing Measles outbreaks
Those exposed through international travel to areas where measles is more common
Why are we seeing Measles outbreaks again?
Although Measles was declared eliminated in the U.S. in 2000, outbreaks have returned due to:
Decreased vaccination rates
Misinformation about vaccine safety
Increased international travel to areas where measles is more common
Does the MMR vaccine protect against Measles?
Yes. The MMR vaccine (Measles, Mumps, Rubella) is very effective:
1 dose = ~93% protection
2 doses = ~97% protection
Most children in the U.S. receive:
1st dose at 12–15 months
2nd dose at 4–6 years
Can my baby get the MMR vaccine early?
In outbreak situations or before international travel, infants as young as 6 months old may receive an early dose. Talk to your pediatrician to see if early vaccination is appropriate.
What should I do if my child is exposed to Measles?
If your child is unvaccinated and may have been exposed:
Call your pediatrician immediately
You may be advised to get the MMR vaccine within 72 hours of exposure
In some cases, immune globulin may be offered for temporary protection
Vaccinated children who are healthy are unlikely to need any intervention.
Can vitamin A or cod liver oil prevent or cure Measles?
No. Vitamin A cannot prevent or cure Measles. However, for children already infected, a physician may recommend vitamin A to support recovery and prevent complications like blindness. Do not self-administer large doses—excess vitamin A can be harmful.
How can I protect my unvaccinated baby from Measles?
If your baby is too young for vaccination:
Avoid crowded places and public transport during outbreaks
Keep sick visitors away
Ensure all caregivers are vaccinated, including grandparents and older caregivers born before 1957 who may no longer be immune or have waning natural immunity. Your specific circumstances and concerns can be discussed with your pediatrician for tailored guidance.
Practice excellent hygiene: handwashing, disinfecting surfaces, covering coughs/sneezes
Continue breastfeeding if possible for added immune support
Ask your pediatrician about early MMR if travel or exposure risk is high
If I was vaccinated, am I protected from Measles?
Most likely. If you received 2 doses of MMR, you’re considered protected. If unsure, check your records or speak with your doctor. Adults born before 1957 are generally considered immune due to likely natural exposure, but they should speak with their physician to better understand their individual circumstances.
Where can I find reliable information about Measles?
Turn to trusted sources, such as:
Your child’s pediatrician
Centers for Disease Control and Prevention (CDC)
World Health Organization (WHO)
National Institutes of Health (NIH)
Local health departments
At Concierge Pediatrics, our board-certified pediatricians are here to answer your questions and help protect your family. Want more information on Measles? Read our blog.
Need help understanding your child’s vaccination status?
We’re here for you. If you’re a Concierge Pediatrics member or parent seeking guidance, give us a call. Your child’s safety and well-being are our top priority.
Strep Throat FAQ for Parents: Symptoms, Treatment & What to Know
What is strep throat?
Strep throat is a bacterial infection of the throat and tonsils caused by Group A Streptococcus. It leads to a sore, red throat, and is most common in children between 5 and 15 years old.
How is strep throat different from a regular sore throat?
Most sore throats are caused by viruses, not bacteria. Only about 30% of sore throats in kids are strep. Unlike viral sore throats, strep:
Typically does not cause a cough or runny nose
Can be treated with antibiotics
May lead to complications if untreated for long periods of time
What are the symptoms of strep throat in children?
Look for these signs:
Sudden sore throat with red, swollen tonsils
Fever
Pain when swallowing
White patches on the throat or tonsils
Swollen glands in the neck
Stomach pain
Bad breath without explanation
No cold symptoms (like coughing or congestion)
How is strep throat diagnosed?
Diagnosis can only be made through:
A rapid strep test (results in minutes)
A throat culture (results in 24–48 hours if the rapid test is negative)
At Concierge Pediatrics, both tests are done in-house for quick and accurate results.
Should toddlers be tested for strep?
Usually, no. Children under 2–3 years old rarely get strep. Testing may be done if:
They’ve had close contact with someone who tested positive
Symptoms are severe or unusual (rash, high fever, difficulty swallowing)
A pediatrician sees cause for concern during an exam
Is strep throat contagious?
Yes. Strep spreads through respiratory droplets from coughing, sneezing, or sharing utensils. It can take 2–5 days after exposure for symptoms to appear.
How is strep throat treated?
Strep throat is treated with antibiotics, most commonly amoxicillin. Treatment helps:
Shorten the duration of illness
Prevent serious complications like rheumatic fever or kidney problems
Reduce the risk of spreading the infection
It’s critical to finish the entire course of antibiotics even if your child feels better.
Can antibiotics cause side effects?
Yes. Common mild side effects include:
Upset stomach
Diarrhea
Yeast infections
Probiotics (like those in Greek yogurt) can help restore gut balance. Call your pediatrician if symptoms are bothersome — and seek immediate care if your child has trouble breathing, facial swelling, or hives.
When can my child return to school or daycare?
Children with strep throat can return to school or other activities after 24 hours of antibiotics, as long as they’ve also been fever-free for 24 hours and are feeling better.
How can I help my child feel better at home?
In addition to antibiotics, try:
Warm saltwater gargles
Fluids, especially warm drinks
Acetaminophen or ibuprofen for pain or fever
Rest
Soft foods to avoid throat irritation
Can my child get strep more than once?
Yes. Some kids get strep multiple times a year. Children who frequently test positive might be strep carriers (they have the bacteria but no symptoms) or in rare cases, may be candidates for a tonsillectomy. Talk to your pediatrician or an ENT specialist if infections are frequent.
What is Scarlet Fever?
Scarlet Fever is a reaction to strep where, in addition to typical symptoms, your child may develop:
Scarlet Fever is a reaction to strep where, in addition to typical symptoms, your child may develop:
A bright red rash
A “strawberry” tongue
Scarlet Fever was once a worrisome disease but is easily treated with antibiotics today.
What is PANDAS and should I be concerned?
PANDAS stands for Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections. Most researchers believe that PANDAS is an autoimmune reaction (i.e., the child’s immune system overreacting to the strep infection) that can appear during childhood, usually between 3 years old and the age of puberty.
It’s a very rare condition where strep may trigger sudden behavioral changes, such as:
Obsessive-compulsive behavior
Tics
Anxiety or mood swings
Can I test for PANDAS?
There is no specific laboratory test to diagnose PANDAS – it is a diagnosis based on experience and the clinical examination of the healthcare provider, and it remains controversial. At Concierge Pediatrics, we can check 2 strep titers in the blood which, if high, is consistent with recent strep infection. If having new onset behavioral issues, this can help us can point to a possible PANDAS situation. It can be treated with cognitive behavioral therapy and sometimes medication. Importantly, a full course of antibiotics must be taken to eliminate the streptococcus infection that may have been the cause.
There are many impassioned conversations among parents regarding PANDAS but it is important to speak directly with your pediatrician about any concerns you may have, to ensure you receive accurate and evidence-based information and an appropriate path forward for your child based on their personal history and circumstances. If you notice unusual symptoms after a strep infection, talk with your pediatrician.
How can I prevent my child from getting strep throat?
Teach good hygiene:
Wash hands regularly
Don’t share drinks or utensils
Cover coughs and sneezes with elbows
When should I call the doctor?
Contact your pediatrician if:
Your child has a sore throat with fever or trouble swallowing
Symptoms don’t improve after starting antibiotics
Your child has a severe reaction to medication
Behavioral changes follow a strep infection
Still have questions?
At Concierge Pediatrics, we’re here to provide evidence-based answers and expert support every step of the way. Contact us directly to become a member or book a sick visit for fast, compassionate care. Want more information on Strep throat? Read our blog.
Sunscreen protects your child’s skin from harmful UV rays, reducing the risk of:
Sunburn
Skin damage
Premature aging
Skin cancer (even though it’s rare in children)
Applying sunscreen daily builds healthy habits that last a lifetime.
What kind of sunscreen should I use?
Look for these three features:
Broad Spectrum – protects against both UVA and UVB rays
SPF 30 or higher – the American Academy of Dermatology recommends SPF 30+
Water Resistant – for pool days, beach trips, and sports
What does SPF mean?
SPF stands for Sun Protection Factor. It measures how well sunscreen protects your skin from sunburn caused by UVB rays. Important: SPF does not tell you how long you can stay in the sun. Reapply sunscreen every 2 hours, or after swimming, sweating, or toweling off.
What’s the difference between mineral and chemical sunscreens?
Mineral sunscreen (like zinc oxide, titanium dioxide, etc.) sits on the skin and reflects UV rays as a physical barrier. It’s gentle for babies and kids with sensitive skin.
Chemical sunscreen (like oxybenzone, octinoxate, etc.) absorbs into the bloodstream, blocking UV rays. It’s effective, but some parents prefer to avoid it due to potential hormone concerns.
Both types are safe and effective when used correctly.
Are there ingredients I should avoid?
Consider limiting products with oxybenzone for young children. While FDA-approved, studies suggest it may affect hormone development. If no other sunscreen is available, it is OK to use sunscreen containing this ingredient, as it is safer than going without sunscreen. When in doubt, choose zinc oxide or titanium dioxide—both are considered safest by the FDA and environmentally friendly.
Is sunscreen safe for babies?
Under 6 months: Avoid direct sunlight. Use shade and protective clothing instead.
6 months and older: You can safely apply mineral sunscreen on exposed skin.
Where should I apply sunscreen?
Apply 15 minutes before sun exposure to all exposed areas, including:
Face (don’t forget eyelids and lips)
Ears
Back of neck
Tops of feet
Hands
Scalp (especially with thinning hair or part lines)
Behind knees and under straps or swimsuit edges
How often should I reapply sunscreen?
Every 2 hours
After swimming, sweating, or toweling off
Even water-resistant sunscreen needs to be reapplied regularly.
Can sunscreen cause cancer?
No. Sunscreen does not cause cancer. In fact, it protects against the harmful UV rays that are proven to cause skin cancer. Online misinformation exists, but no credible studies support this claim.
How can I protect my child beyond sunscreen?
Sun safety also means:
Avoiding peak sun hours (10am–3pm)
Staying in the shade
Wearing wide-brimmed hats and UV-protective clothing
Staying hydrated
Does sunscreen block vitamin D?
Yes, sunscreen reduces vitamin D absorption—but not completely, especially if any part of your body is exposed to the sun without protection. Your child can get vitamin D through:
15–30 minutes of sun exposure in April – October in the northeastern United States
Foods like eggs, fortified milk, yogurt, cereal, and fatty fish
Supplements (ask your pediatrician before starting)
Is it true that a base tan prevents sunburn?
No. A “base tan” does not protect your skin. Any tan or burn is a sign of skin damage. The best skin is protected skin.
What if my child gets sunburned?
For mild sunburn:
Use aloe vera
Apply cool compresses
Give acetaminophen (per dosing guidelines) for discomfort
Call your pediatrician if your child has:
Blisters
Fever, chills, vomiting
Severe pain or heat exhaustion signs
How can I tell if a mole is concerning?
Use the ABCDE Rule:
Asymmetry – one half doesn’t match the other
Border – irregular or jagged edges
Color – multiple or uneven colors
Diameter – larger than a pencil eraser (6mm)
Evolving – changes in size, color, or shape
If you notice anything unusual, schedule a skin check with your pediatrician or dermatologist.
Need Help Choosing the Right Sunscreen?
We’re here to support your family with trusted advice. Ask your pediatrician at Concierge Pediatrics for product recommendations that fit your child’s skin type and your lifestyle.
Still have questions?
At Concierge Pediatrics, we’re here to provide evidence-based answers and expert support every step of the way. Contact us directly to become a member or book a sick visit for fast, compassionate care.
As parents, we want our children to grow up curious, connected, and emotionally healthy. But in a world filled with screens, ever-evolving social media, and a seemingly endless supply of dopamine-inducing content being served to our kids online, knowing how to protect our children and taking a modern approach can leave parents and caregivers feeling confused.
A recent study was published by the American Psychological Association, in which researchers conducted a meta-analysis of 117 studies of nearly 300,000 children across the world, revealing that too much screentime can lead to emotional and behavioral problems. This was especially prevalent in school aged children 6-10 years old, and a more significant impact was noted among girls of that age group.
So how do parents balance appropriate limitations to screen time while living in a modern world?
“How much screen time is too much?”
There is no one-size-fits-all option, as this is dependent on how your child and family interact with their devices, what content is being engaged, and how easy it is to put the device down. It has been generally recommended, however, to avoid screens (other than human engagement on a video call) for babies under age 2, as they learn best by exploring the world around them and interacting with other people. Most importantly, for all other ages, it is recommended to consider the quality of the content engagement over only looking at the time spent.
CommonSenseMedia, a non-profit organization that provides age-based ratings and reviews for media, categorizes screen time into 4 categories
To help you plan for your family, the American Academy of Pediatrics developed the 5 C’s of media use. When deciding what is right for your family, consider these 5 things:
Child
Who is your child and what are they like? How do they utilize their media devices? Are they exhibiting any anxiety or behavioral issues? Knowing your child’s individual situation will help you take next steps.
Content
What is your child engaging with on their screen?Do they use social media, watch educational videos, play games, a mix of it all? Are they scrolling, interacting, speaking with people they know or don’t know? What is the content like? Educational? Violent? Rude? Setting unrealistic expectations? Does the content have an end-point or is it designed for nonstop use? Understanding what your child is currently engaging with, as well as what they like to do, will help determine your path forward. Common Sense Media is a good place to help build your library of age-appropriate content and find alternatives to the content that is not benefiting your child.
Calm
How does your child chill out or fall asleep? If devices are how they unwind, and turning them off results in a meltdown, consider slowly implementing new methods to reduce their reliance on screens for comfort.
Crowding Out
Is your family screen time dominating time that can be spent doing other beneficial activities, like play time, making friends, family conversation, education, or sleep? Games, videos, and social media have a lot of ways to keep your child engaged on their devices – longer than they may have planned for – without them even noticing. Take this into account for your family screentime plan.
Communication
Make discussion about responsible use of media, screens, and time a regular conversation in your house. Ongoing, low-stakes conversation (not only when it becomes a problem) about responsible use will keep behaviors in check, and help children be mindful about their time spent by pausing to make better decisions over time. They may not always get it right, but ongoing communication is good intervention. Consider making a family media plan together. The American Academy of Pediatrics offers a tool to help you do this, linked here.
Can screentime be beneficial?
Yes! Our screen devices open our lives up to a worldwide library of information, creativity, and human connection. Screens can also help us engage with loved ones who we may not be able to see in person. The keys to safe screentime are moderation, curation of content, and boundaries. Seek out educational and interactive content, like puzzles, quizzes, creative outlets, reading, or language learning. Not sure where to start? Websites like Commonsensemedia.com, pbs.org, and sesameworkshop.org provide additional guidance for websites and apps suitable for children at various ages.
Tips for Avoiding Screentime dependency
Leave phones, tablets, and TVs outside of the bedroom and charge them in a universal space overnight. If your child needs an alarm clock, the “old-fashioned” kind can still be purchased!
Create a buffer between screen time and bed time. Consider turning off all screen devices at least 30 minutes before a child is expected to go to sleep.
Avoid giving screens when children are expected to be engaging with others, like at meal times or during social events.
Continuously monitor what your child (of any age) is engaging with on their device. With many social apps providing the opportunity to engage with strangers, video streaming services automatically playing new videos, and endless availability of social media, it can be difficult to put devices down.
Make conversations about screentime and responsible media use an ongoing conversation among your family, ensuring that you and other adults in your home also model good behaviors when it comes to media engagement and device use.
What alternatives to screen time are recommended?
Opt for a mix of structured and unstructured play for all ages. Taking a weekly course, sport, or other activity will keep them away from mindless use of screen devices and allow them to build relationships in person. If the activity requires practice, and the child is passionate about the activity, more time can be set aside to practice their skills alone or with a friend.
Unstructured play can be as simple as going out into the backyard, taking a walk, going to a playground, creating art, or playing make-believe. Unstructured play is an activity where the child determines what they will be doing without direct adult guidance, rules, or supervision (other than for safety purposes). Besides taking up time that could otherwise be occupied with a screen, promoting unstructured play time allows children of all ages to come up with their own solutions to combat feelings of boredom. People often turn to devices when they are bored, and unstructured play alternatives can help prevent screens from being the solution to boredom.
Should I throw away our devices?
You don’t have to throw away your devices. The modern solution is to understand your family’s and your child’s individual circumstances and develop guidelines and guardrails in moderation that meets you where you are. Most importantly, lead by example! The boundaries you set for your child should be boundaries that you set for the adults in your home as well. Modeling good behavior sets the foundation for your children to be able to enforce their own healthy behaviors and follow your guidance.
Setting boundaries, introducing educational and beneficial content, and modeling good behaviors will help us to set our children up for success in their emotional and social health. The most important thing to consider for your child and their media use is moderation and quality of digital media intake. Still need help navigating the journey? The pediatricians and team of pediatric professionals at Concierge Pediatrics are here to help you build a roadmap that works for your family.
$300 of Every New Concierge Pediatric Member Goes to Support Sunrise
Sunrise Day Camp–Long Island is excited to announce our newest sponsor Concierge Pediatrics — a membership-based practice, giving patients unprecedented access to their pediatrician, greater convenience with same-day appointments and zero wait times, and the personalized care that its members are looking for from their pediatrician. Concierge Pediatrics is conveniently located at 1520 Northern Blvd in Roslyn, NY.
For every new member that joins Concierge Pediatrics through the end of the year, Sunrise Day Camp Long Island will receive $300 to help bring the joys of childhood back to children battling cancer.